Complete downloaded form
Fax to TARPEYO Touchpoints® at 1-844-854-3251


TARPEYO is contraindicated in patients with hypersensitivity to budesonide or any of the ingredients of TARPEYO. Serious hypersensitivity reactions, including anaphylaxis, have occurred with other budesonide formulations.
When corticosteroids are used chronically, systemic effects such as hypercorticism and adrenal suppression may occur. Corticosteroids can reduce the response of the hypothalamus-pituitary-adrenal (HPA) axis to stress. In situations where patients are subject to surgery or other stress situations, supplementation with a systemic corticosteroid is recommended. When discontinuing therapy or switching between corticosteroids, monitor for signs of adrenal axis suppression.
Patients with moderate to severe hepatic impairment (Child-Pugh Class B and C, respectively) could be at an increased risk of hypercorticism and adrenal axis suppression due to an increased systemic exposure to oral budesonide. Avoid use in patients with severe hepatic impairment (Child-Pugh Class C). Monitor for increased signs and/or symptoms of hypercorticism in patients with moderate hepatic impairment (Child-Pugh Class B).
Corticosteroids, including TARPEYO, suppress the immune system and increase the risk of infection with any pathogen, including viral, bacterial, fungal, protozoan, or helminthic pathogens. Corticosteroids can: reduce resistance to new infections, exacerbate existing infections, increase the risk of disseminated infections, increase the risk of reactivation or exacerbation of latent infections, and mask some signs of infection. Corticosteroid-associated infections can sometimes be serious. Monitor for infection and consider TARPEYO withdrawal as needed.
Avoid corticosteroid therapy, including TARPEYO, in patients with active or quiescent tuberculosis or hepatitis B infection; untreated fungal, bacterial, systemic viral, or parasitic infections; ocular herpes simplex; or Kaposi’s sarcoma. Avoid exposure to active, easily transmitted infections (e.g., chickenpox, measles). Corticosteroid therapy may decrease the immune response to some vaccines.
TARPEYO is a systemically available corticosteroid and is expected to cause related adverse reactions. Monitor patients with hypertension, prediabetes, diabetes mellitus, osteoporosis, peptic ulcer, glaucoma or cataracts, or with a family history of diabetes or glaucoma, or with any other condition where corticosteroids may have unwanted effects.
In clinical studies, the most common adverse reactions with TARPEYO (occurring in ≥5% of TARPEYO-treated patients, and ≥2% higher than placebo) were peripheral edema (17%), hypertension (12%), muscle spasms (12%), acne (11%), headache (10%), upper respiratory tract infection (8%), face edema (8%), weight increased (7%), dyspepsia (7%), dermatitis (6%), arthralgia (6%), and white blood cell count increased (6%).
Budesonide is a substrate for CYP3A4. Avoid use with potent CYP3A4 inhibitors, such as ketoconazole, itraconazole, ritonavir, indinavir, saquinavir, erythromycin, and cyclosporine. Avoid ingestion of grapefruit juice with TARPEYO. Intake of grapefruit juice, which inhibits CYP3A4 activity, can increase the systemic exposure to budesonide.
The available data from published case series, epidemiological studies, and reviews with oral budesonide use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. There are risks to the mother and fetus associated with IgAN. Infants exposed to in utero corticosteroids, including budesonide, are at risk for hypoadrenalism.
TARPEYO is indicated to reduce the loss of kidney function in adults with primary immunoglobulin A nephropathy (IgAN) who are at risk for disease progression.


Eligible patients may pay $
for their TARPEYO prescription
Financial support options may be available to reduce or eliminate out-of-pocket costs.*
Fax to TARPEYO Touchpoints® at 1-844-854-3251
Complete the enrollment form online at CoverMyMeds.com
Search for TARPEYO, complete online form, and submit

When prescribing, always select TARPEYO (NDC 81749-004-01). There is no generic equivalent for TARPEYO.
TARPEYO is distributed exclusively through PANTHERx Rare Pharmacy.
Bottle not to scale.


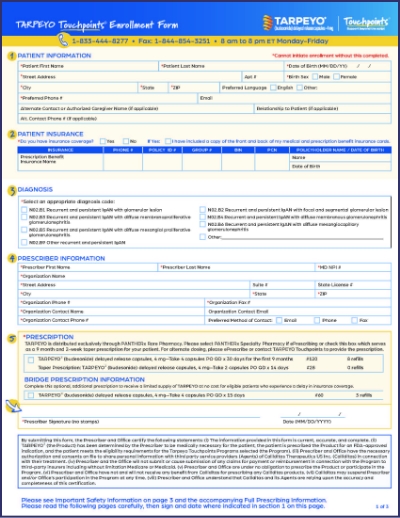
Access the enrollment form and helpful diagnosis codes.


Eligible patients may pay $
for their TARPEYO prescription
Financial support options may be available to reduce or eliminate out-of-pocket costs.*
*Eligibility required. Please view the full terms and conditions.
ACEi=angiotensin-converting enzyme inhibitor; ARB=angiotensin receptor blocker; eGFR=estimated glomerular filtration rate; KDIGO=Kidney Disease: Improving Global Outcomes; UPCR=urine protein-to-creatinine ratio.
TARPEYO is contraindicated in patients with hypersensitivity to budesonide or any of the ingredients of TARPEYO. Serious hypersensitivity reactions, including anaphylaxis, have occurred with other budesonide formulations.
When corticosteroids are used chronically, systemic effects such as hypercorticism and adrenal suppression may occur. Corticosteroids can reduce the response of the hypothalamus-pituitary-adrenal (HPA) axis to stress. In situations where patients are subject to surgery or other stress situations, supplementation with a systemic corticosteroid is recommended. When discontinuing therapy or switching between corticosteroids, monitor for signs of adrenal axis suppression.
Patients with moderate to severe hepatic impairment (Child-Pugh Class B and C, respectively) could be at an increased risk of hypercorticism and adrenal axis suppression due to an increased systemic exposure to oral budesonide. Avoid use in patients with severe hepatic impairment (Child-Pugh Class C). Monitor for increased signs and/or symptoms of hypercorticism in patients with moderate hepatic impairment (Child-Pugh Class B).
Corticosteroids, including TARPEYO, suppress the immune system and increase the risk of infection with any pathogen, including viral, bacterial, fungal, protozoan, or helminthic pathogens. Corticosteroids can: reduce resistance to new infections, exacerbate existing infections, increase the risk of disseminated infections, increase the risk of reactivation or exacerbation of latent infections, and mask some signs of infection. Corticosteroid-associated infections can sometimes be serious. Monitor for infection and consider TARPEYO withdrawal as needed.
Avoid corticosteroid therapy, including TARPEYO, in patients with active or quiescent tuberculosis or hepatitis B infection; untreated fungal, bacterial, systemic viral, or parasitic infections; ocular herpes simplex; or Kaposi’s sarcoma. Avoid exposure to active, easily transmitted infections (e.g., chickenpox, measles). Corticosteroid therapy may decrease the immune response to some vaccines.
TARPEYO is a systemically available corticosteroid and is expected to cause related adverse reactions. Monitor patients with hypertension, prediabetes, diabetes mellitus, osteoporosis, peptic ulcer, glaucoma or cataracts, or with a family history of diabetes or glaucoma, or with any other condition where corticosteroids may have unwanted effects.
In clinical studies, the most common adverse reactions with TARPEYO (occurring in ≥5% of TARPEYO-treated patients, and ≥2% higher than placebo) were peripheral edema (17%), hypertension (12%), muscle spasms (12%), acne (11%), headache (10%), upper respiratory tract infection (8%), face edema (8%), weight increased (7%), dyspepsia (7%), dermatitis (6%), arthralgia (6%), and white blood cell count increased (6%).
Budesonide is a substrate for CYP3A4. Avoid use with potent CYP3A4 inhibitors, such as ketoconazole, itraconazole, ritonavir, indinavir, saquinavir, erythromycin, and cyclosporine. Avoid ingestion of grapefruit juice with TARPEYO. Intake of grapefruit juice, which inhibits CYP3A4 activity, can increase the systemic exposure to budesonide.
The available data from published case series, epidemiological studies, and reviews with oral budesonide use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. There are risks to the mother and fetus associated with IgAN. Infants exposed to in utero corticosteroids, including budesonide, are at risk for hypoadrenalism.
TARPEYO is indicated to reduce the loss of kidney function in adults with primary immunoglobulin A nephropathy (IgAN) who are at risk for disease progression.
