


Managing and treating IgAN



Filter:

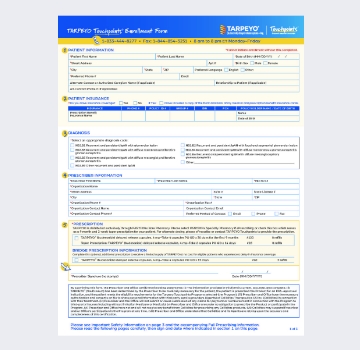
CoverMyMeds® Form
An electronic enrollment
form through CoverMyMeds
to help get your patients
started on TARPEYO.
KDIGO 2025 Guideline
A comprehensive overview
of
the most up-to-date
KDIGO 2025
guideline.

MOA Video
A concise, informative
video
illustrating the
unique
mechanism of action of
TARPEYO.

TARPEYO: Reducing Kidney Function Loss in IgAN Video
An overview of IgAN and its potential long-term clinical impact, along with an examination of the Phase 3 NefIgArd trial and outcomes.
WATCH VIDEO
Key Clinical Highlights Video
An overview of TARPEYO clinical evidence, including efficacy, safety, and product design.
WATCH VIDEO
IgAN Guidelines Update: TARPEYO in Clinical Practice
Hear from experts on the 2025 KDIGO guideline, their clinical impact, and the role of TARPEYO in the evolving treatment landscape.
WATCH VIDEO
Discovering TARPEYO,an FDA-approved treatment for IgAN to reduce
the loss of kidney function

Filter:
Patient Brochure
An informative brochure offering essential details about IgAN and TARPEYO.

Help Take Control of IgAN with TARPEYO Video
This webinar explores IgAN as well as how TARPEYO may help preserve the kidney function of people living with IgAN.
WATCH VIDEO
Doctor Discussion Guide
A guide to help patients prepare for informed discussions with their doctor about TARPEYO and how it can address their IgAN.

IgA Nephropathy Foundation
A patient-centric organization for patients and caregivers focused on finding a cure for IgAN.

Filter:
Efficacy
TARPEYO is the only FDA-approved treatment shown to stabilize eGFR while on therapy in a Phase 3 IgAN trial1-3
Results showed:
- Statistically significant difference of 5.05 mL/min/1.73 m2 at 2 years in favor of TARPEYO vs placebo1*
- LS mean change in eGFR of +1.5 mL/min/1.73 m2 at 9 months1
TARPEYO demonstrated >50% less kidney function loss at 2 years1,2 †
The favorable effect of TARPEYO on eGFR was seen as early as month 3 and remained consistent over 2 years.1 The effect of TARPEYO on the long-term rate of decline in kidney function has not been established.1
Check out more information about the efficacy of TARPEYO*The primary endpoint for the interim analysis was UPCR at 9 months compared to baseline (N=199).1†Not all patients in the full analysis set (FAS) contributed data at each time point.1
TARPEYO demonstrated significant reduction with a 9-month fixed course of TARPEYO treatment1
- 52% reduction in UPCR was achieved at 12 months1
- Substantial reduction in UPCR occurred between months 6 and 12, with a 28% difference between these time points1
- Patients in the NefIgArd trial started to see reductions in proteinuria at month 6 and responses deepened through month 121
- Evaluate therapy response at or after month 6 as this is when patients started to see reductions in proteinuria1
- Patients should complete the full 9-month course of therapy to see the full clinical benefits1
- Nearly 2 out of 3 patients who completed a 9-month course of TARPEYO had at least a 30% reduction in UPCR vs baseline2
- With a full course of therapy, 45% of patients had at least a 50% reduction in proteinuria in the TARPEYO group by month 122
Reductions in Gd-IgA1 were seen with TARPEYO.4*
In the NefIgArd study, serum Gd-IgA1 was significantly reduced at months 3, 6, and 9.4,5 NefIgArd is a randomized, double-blind, placebo-controlled, 2-year, Phase 3 trial.4
Data are exploratory. Clinical significance has not been established. Small sample sizes of a specific patient group are limitations of these analyses. Additional longitudinal studies of more diverse patient cohorts are needed to validate findings.
Modulating Gd-IgA1, a key pathogenic biomarker, supports a potential disease-modifying approach to IgAN.5,6
Discover more about the importance of lowering Gd-IgA1*Data from Part A of the Phase 3 NefIgArd trial.
Safety
TARPEYO has an established safety profile1
The majority of adverse reactions were mild or moderate1
Incidence of TESAEs with TARPEYO + RASi vs RASi alone was (9% vs 5%)2
Find out more about the safety profile of TARPEYOTARPEYO has an established safety profile1
The majority of adverse reactions were mild or moderate1
In the NefIgArd study:
- <10% of patients treated with TARPEYO + RASi discontinued due to TEAEs (9% vs 2%)2*
- Most adverse reactions occurring at a greater incidence in the TARPEYO + RASi group were consistent with hypercortisolism and resolved within 3 months after discontinuation1
- Common steroid-specific TEAEs developed at a mean of 4 months following treatment initiation, and generally resolved following treatment cessation8
Clinical events typically seen with systemic corticosteroids were generally limited1,2
- Median change in body weight from baseline did not exceed 2.2 lbs and returned to baseline within 3 months after the end of treatment2
- Median changes in systolic and diastolic blood pressure were small and resolved to baseline levels within 3 months after the end of treatment2†‡
- HbA1c was generally unchanged throughout treatment. Increases in HbA1c observed during treatment generally resolved after the end of treatment2
Incidence of infections was comparable between treatment groups2
- Incidence of infections: TARPEYO + RASi (37.4%); RASi alone (33.5%)2
- Low rates of severe infections requiring hospitalization: 3 (1.5%) TARPEYO + RASi vs 1 (0.5%) RASi alone2,6
No clinically relevant differences between treatment groups in blood pressure, body weight, HbA1c, or creatinine excretion observed6
Find out more about the safety profile of TARPEYO*Safety updated based on NefIgArd Safety Analysis Set, which included data from all patients who received ≥1 dose of study drug. In the global study, an additional 29 patients were enrolled in China for regulatory requirements after global recruitment had ended. ADRs or ARs were reported in the placebo-controlled 9-month treatment period until 14 days after completion of the tapering period.2
†A small numerical increase in median HbA1c levels was observed during TARPEYO treatment, with some outliers evident. Increases occurred in a few TARPEYO-treated patients with a diabetes diagnosis pre-enrollment or with baseline values indicative of pre-diabetes per ADA-defined thresholds (HbA1c 5.7% or FBG 100 mg/dL).2
TARPEYO is not subject to an FDA-required REMS program.1
TARPEYO has no FDA-mandated drug monitoring or vaccine requirements beyond usual care.1
Product Design
TARPEYO is the first and only FDA-approved treatment for IgA nephropathy to reduce the loss of kidney function1
The medication is a targeted-release capsule designed to deliver budesonide directly to a key site of Gd-IgA1 production.2
Learn more about how Tarpeyo worksBudesonide was selected to limit systemic exposure
- Budesonide is a locally acting glucocorticoid designed to limit systemic exposure of first-pass liver metabolism2
- In pharmacokinetic studies comparing TARPEYO and Entocort, TARPEYO exhibited higher maximum plasma concentrations of budesonide while having a shorter terminal half-life, indicating a shorter duration of systemic exposure to budesonide9
Clinical significance is unknown.
- Developed for topical use on mucosal surfaces, budesonide exhibits rapid absorption and prolonged retention in mucosal tissue2
It has not been established to what extent the efficacy of TARPEYO is mediated via local effects in the ileum vs systemic effects.
Learn more about budesonideTARPEYO is a targeted-release capsule designed to deliver budesonide to a key site of Gd-IgA1 production2
Data suggest that TARPEYO is not interchangeable with systemic glucocorticoids or other budesonide products10
- In pharmacokinetic studies comparing TARPEYO and Entocort, TARPEYO exhibited higher maximum plasma concentrations of budesonide while having a shorter terminal half-life, indicating a shorter duration of systemic exposure to budesonide10
Clinical significance is unknown.
Discover more about what makes TARPEYO uniqueAdministration
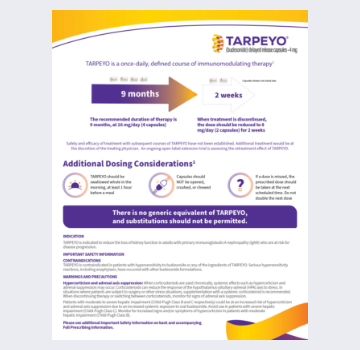
TARPEYO is a once-daily, defined course of immunomodulating therapy.1
The recommended dose for TARPEYO is 16 mg/day (4 capsules). The medication should be swallowed whole in the morning, at least 1 hour before a meal.1
Learn more about determining the correct TARPEYO dose for your patientsThe recommended duration of therapy is 9 months.
When treatment is discontinued, dose should be reduced to 8 mg/day (2 capsules) for 2 weeks.1
Safety and efficacy of treatment with subsequent courses of TARPEYO have not been established. Additional treatment would be at the discretion of the treating physician. An ongoing open-label extension trial (NCT04541043) is assessing the retreatment effect of TARPEYO.
If a dose is missed, the prescribed dose should be taken at the next scheduled time. Do NOT double the next dose.1
Financial support options are available to reduce or eliminate out-of-pocket costs.*
97% of TARPEYO patients have paid less than $10 per prescription*
TARPEYO Touchpoints will explore financial support options for your patients to reduce or eliminate their out-of-pocket costs
Steps to enroll patients in TARPEYO Touchpoints:
- Step 1: Complete the Enrollment Form
- ° Fill out required fields marked with a red asterisk (*)
- ° Both patient and prescriber must sign and date the enrollment form
- Step 2: Include Supporting Documents
- ° Prescription benefit insurance information (front and back of card)
- ° Recent lab results, including UPCR and eGFR
- ° Kidney biopsy documentation
- ° Clinical notes, including current and past medications
- ° ACEi/ARB and dates of any previous steroid use
- Step 3: Fax the completed form
- ° Fax the completed form and supporting information to 1-844-854-3251
- ° Pharmacy Name: PANTHERx Rare Pharmacy
- ° Pharmacy Address: 24 Summit Park Dr, Pittsburgh, PA 15275
You will receive a follow-up phone call from a TARPEYO Touchpoints Care Navigator
Touchpoints will begin the benefits investigation
Touchpoints will fill the prescription through PANTHERx Rare Pharmacy and arrange for home delivery directly to your patientʼs doorstep
Touchpoints will provide ongoing support to your patients during their treatment journey
Learn more about Touchpoints*All patients regardless of insurance type. This includes Commercial, Medicare, Medicaid, and cash-paying patients from January 2024.
Engage with us directly
Request tailored information and guidance from a Calliditas Representative.